As the saying goes, if this journey was easy, anyone would do it. That is precisely why you are unique. You are the chosen one to have that innate drive to keep pushing to get where you need to be. Sure, the road is long, but life is long. A long journey should never be your excuse for not pursuing a career of your choice. Now imagine getting up on that stage to receive your first white coat. Keep envisioning and keep dreaming.
And remember! It is okay to fail. As I mentioned in my previous post, failing a class did not stop me! It just helped me reevaluate my weaknesses. I referenced someone for help and realized that I was studying wrong the whole time during my first semester of college.
Keep pushing! You got this! #girlstrong
Circa 2019, as a 4th-year medical student doing my clinicals in dermatology. I did not match into dermatology, but that is a topic for later discussion. The journey never ends, and you will still fail throughout. But you must always maintain that grit that got you into medicine in the first place. I felt sad and alone here. But I never quit or once doubted my decision to become a doctor.
Whether or not this is a necessary thing to do, I always start my MICU progress notes with a summary of the events that have occurred since hospitalization. I will update this section when significant events occurred.
Example: This is a 46-yo F with a history of type 1 diabetes who is on day 1 of hospitalization and presented with nausea and vomiting. On presentation, the patient was found to have an anion-gap metabolic acidosis with ketonuria and was admitted to the MICU for management of diabetic ketoacidosis with insulin gtt, and frequent lab draws. Since admission, her anion gap has closed and was bridged with subcutaneous insulin.
I think if a resident can summarize the chief complaint and what we are treating, then ICU becomes a heck of a lot easier. When you struggle on your ICU rotation, remember to ask yourself, “what are we treating” and “why is this person sick?”
Common mistakes
Copying and pasting incorrect information
Not updating important events that took place
Listing out every possible past medical history that is not relevant to the case and fluffing the sentences
24-Hour Course
In this section, I like to add everything that has happened over the last 24 hours. I write out my 24-hour events the same way every single time.
Subjective: What the patient said, what the nurse said, any events overnight)
Vitals: Are they hemodynamically stable? If not, how is their hemodynamics managed?
Example: Patient remains afebrile over 24 hours, requiring Levophed 15 mcg and vasopressin for hemodynamic support.
Intake and Output: This is especially important for ICU patients as they are critically ill and, more times than not, if ignored, can easily become under or over-resuscitated. Please obtain accurate intake and output every single day.
Labs: I do not list out values; I state what those values mean.
Example 1: Instead of writing Na+ 121 with an osmolarity of 230, I will write hyperosmolar hyponatremia.Example 2: If the values are significant, like renal functioning, and we are trending the values, sometimes I will write out relevant information only. Side note: You will lose your attending if you just rattle off and list a bunch of lab values. This can be done in the lab section if you wish to reiterate the significant lab findings.
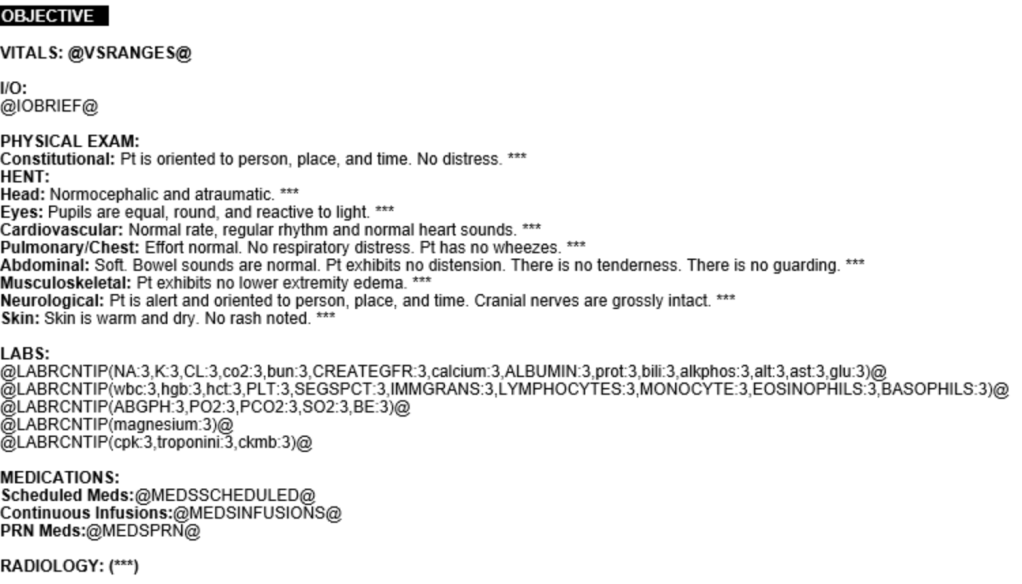
The program I use is EPIC. This is more or less how a template will appear. The *** means you cannot sign your note unless you address that section.
Objective
Vitals
Record vitals over 24 hours. Ensure you indicate episodes of tachyarrhythmias or bradyarrhythmia. Not the times when vitals change. Consider why those values are changing (i.e., is the patient agitated, is the patient in pain, do they have a lead wire that accidentally activates the SA node?)
Intake/Output
In brief, I want to reiterate the importance of fluid balance in the ICU. Once again, one needs to ask themselves, “where is the fluid going.” If you notice that your patient is +15 L and cannot be weaned from the ventilator, chances are there is a problem, which is wet lungs, for example.
Physical Exam
You can still do a complete physical examination on an ICU patient. For example, if a patient is sedated and intubated, a neurological exam can still be performed. Please check the pupillary, corneal, gag, respiratory, and other reflexes every morning. This is essential in patients who have been ventilated for more than a few days.
Electrolytes
I want to briefly touch on the importance of electrolyte balance in critically ill patients, especially when uncommunicative.
Sodium: Ensure the patient is receiving enough water to prevent hypernatremia (more on this topic later)
Potassium: Values should stay above 4 mmol/L to 4.5 mmol/LMagnesium: Values should be >2 mEq/L
Phosphorous: Looking at these values is especially true in our patient population, where the majority are from a nursing home fed through PEG tubes. Thus, one must be aware of refeeding syndrome and should ensure phosphorous levels are adequate.
Relevant Imaging
List out any relevant imaging that will help round out the case. A common mistake I hear is when someone reads aloud an impression from a radiologist without first trying to make their own impression regarding the imaging. You are not expected to be a radiologist, but at least make the effort to look at the images.
Demonstrating the use of coding to auto-populate notes so the provider can save time on documentation.
Assessment and Plan
Very different than a typical ward patient hospitalist patient. If you have ever been on pediatric rotation, it is similar in that ICU patients are assessed by systems. Why? Because patients in the ICU have multiple systems involved and must be addressed so that nothing gets overlooked. Get in the habit of writing your notes the same way every day. This will allow your brain to think in an organized fashion. Below is a sample of the template that I follow.
Neuro: #Diagnosis* Assessment
Plan
Example Neuro: #Hepatic encephalopathy His wife reported he was sleeping more often during the day before the presentation. He is AAO x 1, appears disoriented, and has asterixis.
Insert NG tube for medication administration
Ordered lactulose 30 mL tid via NG tube to titrate to a total of 3 bowel movements per day
Below I listed out a sample of the template that I use to help me to remember to add details where it is needed while modifying it to look like the above.
Neurology:
Current RASS: ***, RASS goal: ***
Brain stem reflexes: ***
Sedative requirements: ***
Pain management: ***
Cardiology:
Cardiac rhythm: ***
HR/BP: ***
Vasopressor requirements: ***
MAP goal >65 mmHg
Pulmonary:
Option 1: Patient denies SOB, lungs are clear to auscultation, no acute findings of CXR.
Option 2: Date Intubated: ***; Patient is on mechanical ventilation with mode setting ***, ABG: ***
MAP goal >65 mmHg
Gastroenterology:
Option 1: Patient is on *** diet
Option 2: Tube feeds via *** with *** at *** cc/h.
Nephrology/Electrolytes:
Intake: ***/Output: ***/Net: ***
K+: ***
Mg2+: ***
Infectious Disease:
Abx: *** day ***/***
Endocrinology:
TSH: ***, Hga1c ***% on ***
Insulin regimen: ***
BG goal <180 mg/dL
Hematology:
***
Checklist Manifesto
THE CHECKLIST IS ESSENTIAL! Please do NOT copy and paste this section. Copying and pasting notes are okay to a certain extent but be reminded if you copy and paste material that is not up to date, this can be detrimental to a patient’s care. In addition, if your note is used in court, you may be deemed unreliable as an author if the notes do not reflect your care.
For the record, I got a D- in General Chemistry 1 during my first year of college. There are many reasons for this! One being having no idea how to study! So if you are feeling down about your first semester, this is normal! How did I change the outcome of my fate? I talked to a professor and asked him how I should study. Subjects like algebra, trigonometry, calculus, general chemistry, organic chemistry, and physics all have one thing in common –> Repetition! Act like school is your 8 AM to 5 PM occupation, and utilize that time to answer questions and understand and conceptualize the material. Sometimes a tutor is necessary. But I promise you, even if you do not understand the subject material on the first day, the second day, or even the third day, you WILL eventually understand it if you keep trying.
Here is a photo of me in Ireland after graduating from Florida State University in 2014. My dad died three months before this photo was taken, and I had no idea how I would get into medical school. But hearing his voice in my head made me push forward.
Keep pushing forward. Keep doing the work. Keep showing up.